CMS-1763 PDF Template
Stop searching and find out why people love the ease of creating beautiful and legally compliant CMS-1763 PDF with PDFSimpli.
Stop searching and find out why people love the ease of creating beautiful and legally compliant CMS-1763 PDF with PDFSimpli.
[toc] Medicare covers a good deal of people all over the United States. The program gives low-income and elderly people access to the medical care they wouldn’t be able to afford otherwise. However, sometimes people make the choice to voluntarily stop their Medicare coverage. To voluntarily opt-out, they’ll need to fill out a CMS 1763 form. You are not required to disclose the reason why you are choosing to opt-out of Medicare but you do have the chance to do so.
This request form is the only legal way for a person to terminate their Medicare Plan A or Plan B coverage. Because of how serious this decision is, you’re also required to complete other steps beyond filing the form. In most cases, before the completed form can be submitted, the claimant will have to do an interview with a representative from the Social Security Administration. Said interviews are generally done either on the phone or in person.
The claimant will be required to explain the reasoning behind the decision. After that, the representative from the Social Security office will explain what the insurance termination procedure is going forward. This request is most often made after a person or their spouse finds a job that covers lifetime insurance.
The form is an official document put out by the United States Department of Health and Services. It can be used by any person enrolled in Medicare who wishes to terminate their coverage. Part A plans cover premium hospital stays, while Part B plans cover supplementary health insurance. Such an action of termination has legal grounds in Section 1818A of the Social Security Act.
Medicare is a social insurance program on the federal level. It was developed to provide care to United States citizens over the age of 64, disabled people of any age, and people who suffer from terminal illnesses and are eligible for disability insurance benefits.
Termination of your medical coverage doesn’t have a set due date or strict timeline regulations. A person can file the form whenever they deem it necessary. It should be noted that the termination won’t take place until the end of the month in which the person filed their form.
Retired Americans face certain due dates to apply for the Medicare program. An applicant needs to file their application three months prior to their 65th birthday.
This form is the only means by which a person can voluntarily opt-out of their Medicare insurance benefits. If you don’t use this form, you have no way to opt-out of said insurance benefits.
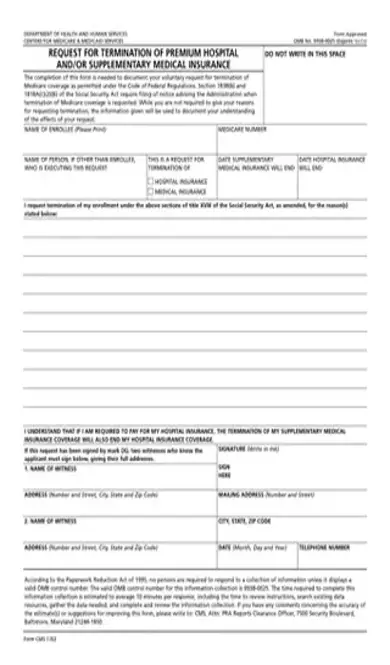
Print your name in the “Name of Enrollee” box, along with your Medicare number. If another person is executing the request, write the name beneath the enrollee’s name.
Print your name in the “Name of Enrollee” box, along with your Medicare number. If another person is executing the request, write the name beneath the enrollee’s name.
Check the box beside the type of coverage you wish to terminate. If you have Plan A, this means you’re terminating your hospital insurance. Plan B is a termination of your medical insurance.
Check the box beside the type of coverage you wish to terminate. If you have Plan A, this means you’re terminating your hospital insurance. Plan B is a termination of your medical insurance.
Write the date when your insurance coverage should end. Plan A enrollees should use the hospital insurance box, while Plan B people should use the supplementary medical insurance box.
Write the date when your insurance coverage should end. Plan A enrollees should use the hospital insurance box, while Plan B people should use the supplementary medical insurance box.
Use the several provided lines to give details about your reason for requesting the coverage termination.
Use the several provided lines to give details about your reason for requesting the coverage termination.
Two witnesses who are familiar with the applicant will be required to sign the document. Box 1 should include the name of the first witness, while their address is printed directly underneath. Box 2 should have the name of the second witness, with their address printed directly underneath. Record the date and telephone numbers of the witnesses. Then have the enrollee sign the form.
That’s all there is to it. The form is fairly straightforward; it’s only one page long, and the majority of that page is empty space you can use to write your reasons.[pdf-embedder url=”https://cdn-prod-pdfsimpli-wpcontent.azureedge.net/pdfseoforms/pdf-20180219t134432z-001/pdf/cms-1763.pdf?sv=2018-03-28&si=readpolicy&sr=c&sig=MXHnWmn0sXNXztiU%2Bugk2d7DV7KBCOuXF3oBMx0EeEw%3D”]
The witnesses should know the enrollee well enough to testify that they are filing the application in sound mind and body. They should also be able to attest that the applicant is making the best decision for themselves.
You should provide as much detail as you’re reasonably able to. If you or your spouse received a job with health insurance benefits, explain the type of job, the type of insurance benefits, and the insurance company you’ll be enrolling with.
If you have coverage for both Plan A and Plan B, you’re welcome to withdraw from both if you wish.
Select Language
© 2026 , WorkSimpli Software, LLC. All rights reserved.