VA 10-5345A PDF Template
Stop searching and find out why people love the ease of creating beautiful and legally compliant VA 10-5345A PDF with PDFSimpli.
Stop searching and find out why people love the ease of creating beautiful and legally compliant VA 10-5345A PDF with PDFSimpli.
[toc] Many individuals have their medical information managed through the Department of Veteran Affairs. There are some cases wherein an individual will request to be given a copy of their own health information. Because this information isn’t kept from the individual, it may seem surprising that there’s an official form for the request. But the request form is the best way to make sure false claims aren’t filed and information isn’t released into the wrong hands.
If the Department of Veteran Affairs is responsible for maintaining your medical information, requests for that information will be handled through them. This is the purpose of the VA Form 10-5345. When you fill out the form, you’ll voluntarily disclose information about yourself. In return, the Department of Veteran Affairs will release the requested medical information.
There are some situations in which the VA is not able to honor a request. If any of the information on the form is incorrect, especially the Social Security Number, the request won’t be able to be verified. However, a failure to furnish any information doesn’t affect any other veteran benefits that you’re entitled to.
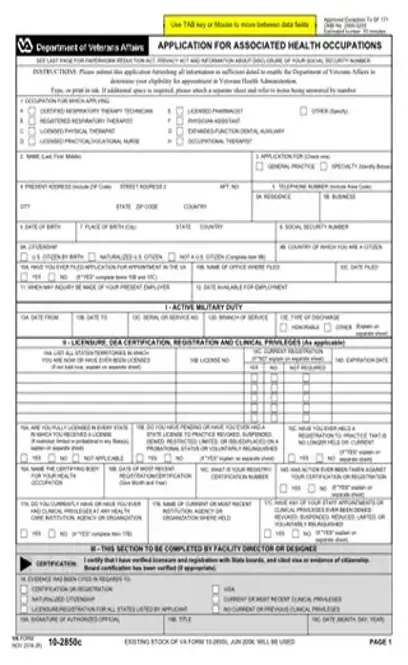
The form will take down basic information about you, like your name, DOB, and the last four numbers of your SSN. You’ll give a description of the information you need. Then, you’ll indicate the method in which a copy of your health information should be delivered to you.
This is a 1-page form. It’s fairly easy to fill out.
[pdf-embedder url=”https://cdn-prod-pdfsimpli-wpcontent.azureedge.net/pdfseoforms/pdf-20180219t134432z-001/pdf/va-form-10-2850c.pdf”]
If a person’s medical records and history are being maintained by the VA, and that person wants a copy of their medical records, this is the form they need to fill out. Information cannot be released unless this form is filed first.
This form should be used if you need a copy of your health information for any reason. Your reasons might include going to a new doctor, needing to search for a preexisting condition, and needing a record of previous tests during a hospital stay. You might also just want to have a copy to keep for your personal records.
There’s a whole host of reasons you might want access to your medical information. Completing this form is the quickest, easiest way to get those records.
If you don’t fill out the form, you can’t receive a copy of your medical records from the VA. They need on-paper documentation that a request was made for the information release. It’s a liability-related measure. Though this may seem like a pain, said measure is put in place to protect your overall privacy.
In the top box, write the name and address of your closest VA healthcare facility.
Write your name, starting with your last name, then your first name, then your middle initial. In the box beside it, clearly print the last 4 digits of your SSN along with your date of birth.
In the “Description of Information Requested” section, check the boxes that verify the information that should be provided. If you check a box with a blank beside it, look at the instructions in parentheses to know what to list there. Some lines need dates, some need name and date ranges, and some need descriptions.
The next section refers to the way that a copy of your health information should be personally delivered to you. You can choose to have it delivered on paper, on a CD-ROM, or in another format. If you intend to pick it up in person, you need to provide a phone number at which you can be contacted. If you want the information mailed instead, you’ll need to provide a mailing address on the appropriate lines.
Sign the form and input the date in MM-DD-YYYY format. If you’re signing the paper on someone else’s behalf, you should indicate what authority you’re using to make the request. Generally, this will be related to power of attorney or guardianship.
You’re free to request any health information that the VA maintains. There’s a good chance that the majority of your medical records, if not all of them, are maintained through the VA. It’s important to have a copy of them when you see new doctors or seek new treatments.
If you don’t need all of your information, the VA will give you whatever you specifically asked for. If you check the box for ‘Health Summary,’ you’ll be given your full medical history report for the past two years.
One of the boxes you can check is for a list of active medications.
Select Language
© 2026 , WorkSimpli Software, LLC. All rights reserved.